Description for Pyzchiva
Ustekinumab-ttwe, a human IgG1κ monoclonal antibody, is a human interleukin-12 and -23 antagonist. Using DNA recombinant technology, ustekinumab-ttwe is produced in a Chinese hamster ovary cell line. The manufacturing process contains steps for the clearance of viruses. Ustekinumab-ttwe is comprised of 1326 amino acids and has an estimated molecular mass that ranges from 148,079 to 149,690 Daltons.
PYZCHIVA (ustekinumab-ttwe) injection is a clear, colorless to light yellow, sterile and preservative-free solution with pH of 5.7– 6.3.
PYZCHIVA For Subcutaneous Use
Available as 45 mg of ustekinumab-ttwe in 0.5 mL and 90 mg of ustekinumab-ttwe in 1 mL, supplied as a sterile solution in a single-dose prefilled syringe with a 29 gauge fixed ½ inch needle. The syringe is fitted with a passive needle guard and a needle cover.
Each 0.5 mL prefilled syringe delivers 45 mg ustekinumab-ttwe, histidine (0.095 mg), histidine hydrochloride monohydrate (0.405 mg), polysorbate 80 (0.02 mg), and sucrose (42.5 mg).
Each 1 mL prefilled syringe delivers 90 mg ustekinumab-ttwe, histidine (0.19 mg), histidine hydrochloride monohydrate (0.81 mg), polysorbate 80 (0.04 mg), and sucrose (85 mg).
PYZCHIVA for Intravenous Infusion
Available as 130 mg of ustekinumab-ttwe in 26 mL, supplied as a single-dose 30 mL Type I glass vial with a coated stopper.
Each 26 mL vial delivers 130 mg ustekinumab-ttwe, edetate disodium (0.52 mg), histidine (20 mg), histidine hydrochloride monohydrate (27 mg), methionine (10.4 mg), polysorbate 80 (10.4 mg) and sucrose (2,210 mg).
Uses for Pyzchiva
Plaque Psoriasis (PsO)
PYZCHIVA is indicated for the treatment of adults and pediatric patients 6 years of age and older with moderate to severe plaque psoriasis who are candidates for phototherapy or systemic therapy.
Psoriatic Arthritis (PsA)
PYZCHIVA is indicated for the treatment of adults and pediatric patients 6 years of age and older with active psoriatic arthritis.
Crohn's Disease (CD)
PYZCHIVA is indicated for the treatment of adult patients with moderately to severely active Crohn's disease.
Ulcerative Colitis
PYZCHIVA is indicated for the treatment of adult patients with moderately to severely active ulcerative colitis.
Dosage for Pyzchiva
Recommended Dosage In Plaque Psoriasis
Subcutaneous Adult Dosage Regimen
- For patients weighing 100 kg or less, the recommended dose is 45 mg initially and 4 weeks later, followed by 45 mg every 12 weeks.
- For patients weighing more than 100 kg, the recommended dose is 90 mg initially and 4 weeks  later, followed by 90 mg every 12 weeks. In subjects weighing more than 100 kg, 45 mg was also shown to be efficacious. However, 90 mg resulted in greater efficacy in these subjects [see Clinical Studies].
Subcutaneous Pediatric Dosage Regimen
Administer PYZCHIVA subcutaneously at Weeks 0 and 4, then every 12 weeks thereafter. The recommended dose of PYZCHIVA for pediatric patients (6–17 years old) with plaque psoriasis  based on body weight is shown below (Table 1).
Table 1: Recommended Dose of PYZCHIVA for Subcutaneous Injection in Pediatric Patients (6–17 years old) with Plaque Psoriasis
| Body Weight of Patient at the Time of Dosing | Recommended Dose |
| 60 kg to 100 kg | 45 mg |
| more than 100 kg | 90 mg |
There is no dosage form for PYZCHIVA that allows weight-based dosing for pediatric patients below 60 kg (132 pounds).
Recommended Dosage In Psoriatic Arthritis
Subcutaneous Adult Dosage Regimen
- The recommended dosage is 45 mg initially and 4 weeks later, followed by 45 mg every 12 weeks.
- For patients with co-existent moderate-to-severe plaque psoriasis weighing more than 100 kg, the recommended dosage is 90 mg initially and 4 weeks later, followed by 90 mg every 12 weeks.
Subcutaneous Pediatric Dosage Regimen
Administer PYZCHIVA subcutaneously at Weeks 0 and 4, then every 12 weeks thereafter.
The recommended dose of PYZCHIVA for pediatric patients (6 to 17 years old) with psoriatic arthritis, based on body weight, is shown below (Table 2).
Table 2: Recommended Dose of PYZCHIVA for Subcutaneous Injection in Pediatric Patients (6 to 17 years old) with Psoriatic Arthritis
| Body Weight of Patient at the Time of Dosing | Recommended Dose |
| 60 kg or more | 45 mg |
| greater than 100 kg with co-existent moderate-to-severe plaque psoriasis | 90 mg |
There is no dosage form for PYZCHIVA that allows weight-based dosing for pediatric patients below 60 kg (132 pounds).
Recommended Dosage In Crohn's Disease And Ulcerative Colitis
Intravenous Induction Adult Dosage Regimen
A single intravenous infusion dose of PYZCHIVA using the weight-based dosage regimen specified in Table 3 [see DOSAGE AND ADMINISTRATION].
Table 3: Initial Intravenous Dosage of PYZCHIVA
| Body Weight of Patient at the time of dosing | Dose | Number of 130 mg/26 mL (5 mg/mL) PYZCHIVA vials |
| 55 kg or less | 260 mg | 2 |
| more than 55 kg to 85 kg | 390 mg | 3 |
| more than 85 kg | 520 mg | 4 |
Subcutaneous Maintenance Adult Dosage Regimen
The recommended maintenance dosage is a subcutaneous 90 mg dose administered 8 weeks after the initial intravenous dose, then every 8 weeks thereafter.
General Considerations For Administration
- PYZCHIVA is intended for use under the guidance and supervision of a healthcare provider. PYZCHIVA should only be administered to patients who will be closely monitored and have regular follow-up visits with a healthcare provider. The appropriate dose should be determined by a healthcare provider using the patient's current weight at the time of dosing. In pediatric patients, it is recommended that PYZCHIVA be administered by a healthcare provider. If a healthcare provider determines that it is appropriate, a patient may self-inject or a caregiver may inject PYZCHIVA after proper training in subcutaneous injection technique. Instruct patients to follow the directions provided in the Medication Guide [see Medication Guide].
- It is recommended that each injection be administered at a different anatomic location (such as upper arms, gluteal regions, thighs, or any quadrant of abdomen) than the previous injection, and not into areas where the skin is tender, bruised, erythematous, or indurated.
- Prior to administration, visually inspect PYZCHIVA for particulate matter and discoloration. PYZCHIVA is a clear, colorless to light yellow, sterile and preservative-free solution. Do not use PYZCHIVA if it is discolored or cloudy, or if other particulate matter is present. PYZCHIVA does not contain preservatives; therefore, discard any unused product remaining in the vial and/or syringe.
Instructions For Administration Of PYZCHIVA Prefilled Syringes Equipped With Needle Safety Guard
Refer to the diagram below for the provided instructions.
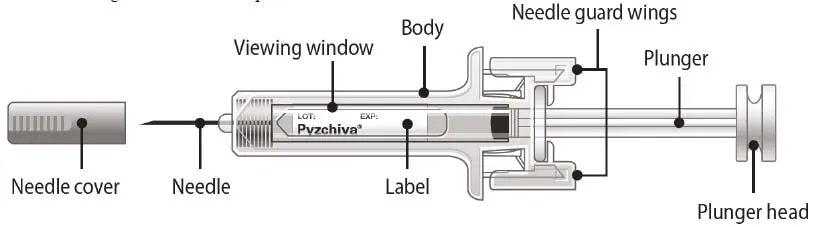 |
- Hold the BODY and remove the NEEDLE COVER. Do not hold the PLUNGER or PLUNGER HEAD while removing the NEEDLE COVER or the PLUNGER may move. Do not use the prefilled syringe if it is dropped without the NEEDLE COVER in place.
- Inject PYZCHIVA subcutaneously as recommended [see DOSAGE AND ADMINISTRATION].
- Inject all of the medication by pushing in the PLUNGER until the PLUNGER HEAD is completely between the needle guard wings. Injection of the entire prefilled syringe contents is necessary to activate the needle guard.
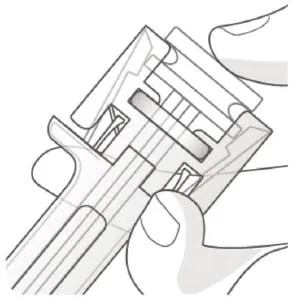 |
After injection, maintain the pressure on the PLUNGER HEAD and remove the needle from the skin. Slowly take your thumb off the PLUNGER HEAD to allow the empty syringe to move up until the entire needle is covered by the needle guard, as shown by the illustration below:
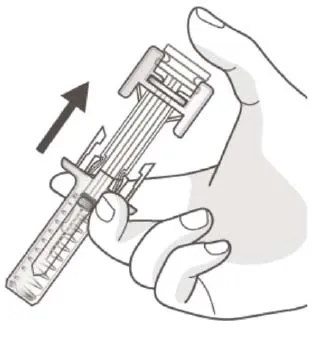 |
- Used syringes should be placed in a puncture-resistant container.
Preparation And Administration Of PYZCHIVA 130 mg/26 mL (5 mg/mL) Vial For Intravenous Infusion (Crohn's Disease and Ulcerative Colitis)
PYZCHIVA solution for intravenous infusion must be diluted, prepared and infused by a healthcare professional using aseptic technique.
- Calculate the dose and the number of PYZCHIVA vials needed based on patient weight (Table 3). Each 26 mL vial of PYZCHIVA contains 130 mg of ustekinumab-ttwe.
- Withdraw, and then discard a volume of the 0.9% Sodium Chloride Injection, USP from the 250 mL infusion bag equal to the volume of PYZCHIVA to be added (discard 26 mL sodium chloride for each vial of PYZCHIVA needed, for 2 vials-discard 52 mL, for 3 vials-discard 78 mL, 4 vials-discard 104 mL). Alternatively, a 250 mL infusion bag containing 0.45% Sodium Chloride Injection, USP may be used.
- Withdraw 26 mL of PYZCHIVA from each vial needed and add it to the 250 mL infusion bag. The final volume in the infusion bag should be 250 mL. Gently mix. Protect from light.
- Visually inspect the diluted solution before infusion. Do not use if visibly opaque particles, discoloration or foreign particles are observed.
- Infuse the diluted solution over a period of at least one hour. Once diluted in the infusion bag, the infusion should be completely administered within 36 hours at room temperature up to 30°C (86°F) .
- Use only an infusion set with an in-line, sterile, non-pyrogenic, low protein-binding filter (pore size 0.2 micrometer).
- Do not infuse PYZCHIVA concomitantly in the same intravenous line with other agents.
- PYZCHIVA does not contain preservatives. Each vial is for a single-dose only. Discard any remaining solution. Dispose any unused medicinal product in accordance with local requirements.
Storage
- The diluted infusion solution may be kept at room temperature up to 30°C (86°F) for up to 36 hours including infusion period.
- If necessary, the diluted infusion solution may be stored refrigerated at 2°C to 8°C (36°F to 46°F) for up to 15 days. After removal from refrigeration, the diluted solution may be stored at room temperature at up to 30°C (86°F) for an additional 24 hours including infusion period. Storage time at refrigerated or room temperature begins once the diluted solution has been prepared. Do not freeze. Protect from light. Discard any unused portion of the infusion solution.
HOW SUPPLIED
Dosage Forms And Strengths
PYZCHIVA (ustekinumab-ttwe) is a clear, colorless to light yellow, sterile and preservative-free solution.
Subcutaneous Injection
- Injection: 45 mg/0.5 mL or 90 mg/mL solution in a single-dose prefilled syringe
Intravenous Infusion
- Injection: 130 mg/26 mL (5 mg/mL) solution in a single-dose vial
Storage And Handling
PYZCHIVA (ustekinumab-ttwe) injection is a clear, colorless to light yellow, sterile and preservative-free solution. It is supplied as individually packaged, single-dose prefilled syringes or single-dose vials.
For Subcutaneous Use
Prefilled Syringes
45 mg/0.5 mL (NDC 61314-651-01)
90 mg/mL (NDC 61314-652-01)
Each prefilled syringe is equipped with a 29 gauge fixed ½ inch needle, a needle safety guard, and a needle cover that is not made with natural rubber latex.
For Intravenous Infusion
Single-dose Vial
130 mg/26 mL (5 mg/mL) (NDC 61314-654-94)
Storage And Stability
Store PYZCHIVA vials and prefilled syringes refrigerated between 2°C to 8°C (36°F to 46°F). Store PYZCHIVA vials upright. Keep the product in the original carton to protect from light until the time of use. Do not freeze. Do not shake.
If needed, individual prefilled syringes may be stored at room temperature up to 30°C (86°F) for a maximum single period of up to 60 days in the original carton to protect from light. If not used within 60 days of room temperature storage, discard the prefilled syringe. The prefilled syringe may be returned to the refrigerator one time only for a maximum of 3 days. If not used within 3 days, discard the prefilled syringe. Record the date when the prefilled syringe is removed from and returned to the refrigerator on the carton in the space provided.
Do not use PYZCHIVA after the expiration date on the carton or on the prefilled syringe.
Manufactured by: Samsung Bioepis Co., Ltd., 76, Songdogyoyuk-ro, Yeonsu-gu, Incheon, 21987, Republic of Korea. Manufactured for: Sandoz Inc. Princeton, NJ 08540. Revised: Jun 2024
Side Effects for Pyzchiva
The following serious adverse reactions are discussed elsewhere in the label:
- Infections [see WARNINGS AND PRECAUTIONS]
- Malignancies [see WARNINGS AND PRECAUTIONS]
- Hypersensitivity Reactions [see WARNINGS AND PRECAUTIONS]
- Posterior Reversible Encephalopathy Syndrome (PRES) [see WARNINGS AND PRECAUTIONS]
- Noninfectious Pneumonia [see WARNINGS AND PRECAUTIONS]
Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Adult Subjects With Plaque Psoriasis
The safety data reflect exposure to ustekinumab in 3117 adult subjects with plaque psoriasis, including 2414 exposed for at least 6 months, 1855 exposed for at least one year, 1653 exposed for at least two years, 1569 exposed for at least three years, 1482 exposed for at least four years and 838 exposed for at least five years.
Table 4 summarizes the adverse reactions that occurred at a rate of at least 1% with higher rates in the ustekinumab groups during the placebo-controlled period of Ps STUDY 1 and Ps STUDY 2 [see Clinical Studies].
Table 4: Adverse Reactions Reported by ≥1% of Subjects with Plaque Psoriasis and at Higher Rates in the Ustekinumab Groups through Week 12 in Ps STUDY 1 and Ps STUDY 2
| Placebo | Ustekinumab 45 mg | 90 mg | |
| Subjects treated | 665 | 664 | 666 |
| Nasopharyngitis | 51 (8%) | 56 (8%) | 49 (7%) |
| Upper respiratory tract infection | 30 (5%) | 36 (5%) | 28 (4%) |
| Headache | 23 (3%) | 33 (5%) | 32 (5%) |
| Fatigue | 14 (2%) | 18 (3%) | 17 (3%) |
| Back pain | 8 (1%) | 9 (1%) | 14 (2%) |
| Dizziness | 8 (1%) | 8 (1%) | 14 (2%) |
| Pharyngolaryngeal pain | 7 (1%) | 9 (1%) | 12 (2%) |
| Pruritus | 9 (1%) | 10 (2%) | 9 (1%) |
| Injection site erythema | 3 (<1%) | 6 (1%) | 13 (2%) |
| Myalgia | 4 (1%) | 7 (1%) | 8 (1%) |
| Depression | 3 (<1%) | 8 (1%) | 4 (1%) |
Adverse reactions that occurred at rates less than 1% in the controlled period of Ps STUDIES 1 and 2 through week 12 included: cellulitis, herpes zoster, diverticulitis and certain injection site reactions (pain, swelling, pruritus, induration, hemorrhage, bruising, and irritation).
One case of PRES occurred during adult plaque psoriasis clinical trials [see WARNINGS AND PRECAUTIONS].
Infections
In the placebo-controlled period of clinical trials of subjects with plaque psoriasis (average follow-up of 12.6 weeks for placebo-treated subjects and 13.4 weeks for ustekinumab-treated subjects), 27% of ustekinumab-treated subjects reported infections (1.39 per subject-year of follow-up) compared with 24% of placebo-treated subjects (1.21 per subject-year of follow-up). Serious infections occurred in 0.3% of ustekinumab-treated subjects (0.01 per subject-year of follow-up) and in 0.4% of placebo-treated subjects (0.02 per subject-year of follow-up) [see WARNINGS AND PRECAUTIONS].
In the controlled and non-controlled portions of plaque psoriasis clinical trials (median follow-up of 3.2 years), representing 8998 subject-years of exposure, 72.3% of ustekinumab-treated subjects reported infections (0.87 per subject-years of follow-up). Serious infections were reported in 2.8% of subjects (0.01 per subject-years of follow-up).
Malignancies
In the controlled and non-controlled portions of plaque psoriasis clinical trials (median follow-up of 3.2 years, representing 8998 subject-years of exposure), 1.7% of ustekinumab-treated subjects reported malignancies excluding non-melanoma skin cancers (0.60 per hundred subject-years of follow-up). Non-melanoma skin cancer was reported in 1.5% of ustekinumab-treated subjects (0.52 per hundred subject-years of follow-up) [see WARNINGS AND PRECAUTIONS]. The most frequently observed malignancies other than non-melanoma skin cancer during the clinical trials were: prostate, melanoma, colorectal and breast. Malignancies other than non-melanoma skin cancer in ustekinumab-treated patients during the controlled and uncontrolled portions of trials were similar in type and number to what would be expected in the general U.S. population according to the SEER database (adjusted for age, gender and race).1
Pediatric Subjects With Plaque Psoriasis
The safety of ustekinumab was assessed in two trials of pediatric subjects with moderate to severe plaque psoriasis. Ps STUDY 3 evaluated safety for up to 60 weeks in 110 pediatric subjects 12 to 17 years old. Ps STUDY 4 evaluated safety for up to 56 weeks in 44 pediatric subjects 6 to 11 years old. The safety profile in pediatric subjects was similar to the safety profile from trials in adults with plaque psoriasis.
Psoriatic Arthritis
The safety of ustekinumab was assessed in 927 subjects in two randomized, double-blind, placebo-controlled trials in adults with active psoriatic arthritis (PsA). The overall safety profile of ustekinumab in subjects with PsA was consistent with the safety profile seen in adult psoriasis clinical trials. A higher incidence of arthralgia, nausea, and dental infections was observed in ustekinumab-treated subjects when compared with placebo-treated subjects (3% vs. 1% for arthralgia and 3% vs. 1% for nausea; 1% vs. 0.6% for dental infections) in the placebo-controlled portions of the PsA clinical trials.
Crohn's Disease
The safety of ustekinumab was assessed in 1407 subjects with moderately to severely active Crohn's disease (Crohn's Disease Activity Index [CDAI] greater than or equal to 220 and less than or equal to 450)in three randomized, double-blind, placebo-controlled, parallel-group, multicenter trials. These 1407 subjects included 40 subjects who received a prior investigational intravenous ustekinumab formulation but were not included in the efficacy analyses. In trials CD-1 and CD-2 there were 470 subjects who received ustekinumab 6 mg/kg as a weight-based single intravenous induction dose and 466 who received placebo [see DOSAGE AND ADMINISTRATION]. Subjects who were responders in either trial CD-1 or CD-2 were randomized to receive a subcutaneous maintenance regimen of either 90 mg ustekinumab every 8 weeks, or placebo for 44 weeks in trial CD-3. Subjects in these 3 trials may have received other concomitant therapies including aminosalicylates, immunomodulatory agents [azathioprine (AZA), 6-mercaptopurine (6-MP), methotrexate (MTX)], oral corticosteroids (prednisone or budesonide), and/or antibiotics for their Crohn's disease [see Clinical Studies].
The overall safety profile of ustekinumab was consistent with the safety profile seen in the adult psoriasis and psoriatic arthritis clinical trials. Common adverse reactions in trials CD-1 and CD-2 and in trial CD-3 are listed in Tables 5 and 6, respectively.
Table 5: Common adverse reactions through Week 8 in Trials CD-1 and CD-2 occurring in ≥3% of ustekinumab-treated subjects and higher than placebo
| Placebo N=466 |
Ustekinumab 6 mg/kg single intravenous induction dose N=470 |
|
| Vomiting | 3% | 4% |
Other less common adverse reactions reported in subjects in trials CD-1 and CD-2 included asthenia (1% vs 0.4%), acne (1% vs 0.4%), and pruritus (2% vs 0.4%).
Table 6: Common adverse reactions through Week 44 in Trial CD-3 occurring in ≥3% of ustekinumabtreated subjects and higher than placebo
| Placebo N=133 |
Ustekinumab 90 mg subcutaneous maintenance dose every 8 weeks N=131 |
|
| Nasopharyngitis | 8% | 11% |
| Injection site erythema | 0 | 5% |
| Vulvovaginal candidiasis/mycotic infection | 1% | 5% |
| Bronchitis | 3% | 5% |
| Pruritus | 2% | 4% |
| Urinary tract infection | 2% | 4% |
| Sinusitis | 2% | 3% |
Infections
In patients with Crohn's disease, serious or other clinically significant infections included anal abscess, gastroenteritis, and pneumonia. In addition, listeria meningitis and ophthalmic herpes zoster were reported in one patient each [see WARNINGS AND PRECAUTIONS].
Malignancies
With up to one year of treatment in the Crohn's disease clinical trials, 0.2% of ustekinumab-treated subjects (0.36 events per hundred patient-years) and 0.2% of placebo-treated subjects (0.58 events per hundred patient-years) developed non-melanoma skin cancer. Malignancies other than non-melanoma skin cancers occurred in 0.2% of ustekinumab-treated subjects (0.27 events per hundred patient-years) and in none of the placebo-treated subjects.
Hypersensitivity Reactions Including Anaphylaxis
In CD trials, two patients reported hypersensitivity reactions following ustekinumab administration. One patient experienced signs and symptoms consistent with anaphylaxis (tightness of the throat, shortness of breath, and flushing) after a single subcutaneous administration (0.1% of patients receiving subcutaneous ustekinumab). In addition, one patient experienced signs and symptoms consistent with or related to a hypersensitivity reaction (chest discomfort, flushing, urticaria, and increased body temperature) after the initial intravenous ustekinumab dose (0.08% of patients receiving intravenous ustekinumab). These patients were treated with oral antihistamines or corticosteroids and in both cases symptoms resolved within an hour.
Ulcerative Colitis
The safety of ustekinumab was evaluated in two randomized, double-blind, placebo-controlled clinical trials (UC-1 [IV induction] and UC-2 [SC maintenance]) in 960 adult subjects with moderately to severely active ulcerative colitis [see Clinical Studies]. The overall safety profile of ustekinumab in patients with ulcerative colitis was consistent with the safety profile seen across all approved indications. Adverse reactions reported in at least 3% of ustekinumab-treated subjects and at a higher rate than placebo were:
- Induction (UC-1): nasopharyngitis (7% vs 4%).
- Maintenance (UC-2): nasopharyngitis (24% vs 20%), headache (10% vs 4%), abdominal pain (7% vs 3%), influenza (6% vs 5%), fever (5% vs. 4%), diarrhea (4% vs 1%), sinusitis (4% vs 1%), fatigue (4% vs 2%), and nausea (3% vs 2%).
Infections
In patients with ulcerative colitis, serious or other clinically significant infections included gastroenteritis and pneumonia. In addition, listeriosis and ophthalmic herpes zoster were reported in one patient each [see WARNINGS AND PRECAUTIONS].
Malignancies
With up to one year of treatment in the ulcerative colitis clinical trials, 0.4% of ustekinumab-treated subjects (0.48 events per hundred patient-years) and 0.0% of placebo-treated subjects (0.00 events per hundred patient-years) developed non-melanoma skin cancer. Malignancies other than non-melanoma skin cancers occurred in 0.5% of ustekinumab-treated subjects (0.64 events per hundred patient-years) and 0.2% of placebo-treated subjects (0.40 events per hundred patient-years).
Immunogenicity
The observed incidence of anti-drug antibodies is highly dependent on the sensitivity and specificity of the assay. Differences in assay methods preclude meaningful comparisons of the incidence of anti-drug antibodies in the studies described below with the incidence of anti-drug antibodies in other studies, including those of ustekinumab or of other ustekinumab products.
Approximately 6 to 12.4% of subjects treated with ustekinumab in plaque psoriasis and psoriatic arthritis clinical trials developed antibodies to ustekinumab, which were generally low-titer. In plaque psoriasis clinical trials, antibodies to ustekinumab were associated with reduced or undetectable serum ustekinumab concentrations and reduced efficacy. In plaque psoriasis trials, the majority of subjects who were positive for antibodies to ustekinumab had neutralizing antibodies.
In Crohn's disease and ulcerative colitis clinical trials, 2.9% and 4.6% of subjects, respectively, developed antibodies to ustekinumab when treated with ustekinumab for approximately one year. No apparent association between the development of antibodies to ustekinumab and the development of injection site reactions was seen.
Postmarketing Experience
The following adverse reactions have been reported during post-approval use of ustekinumab products. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to ustekinumab product exposure.
Immune system disorders: Serious hypersensitivity reactions (including anaphylaxis and angioedema), other hypersensitivity reactions (including rash and urticaria).
Infections and infestations: Lower respiratory tract infection (including opportunistic fungal infections and tuberculosis).
Neurological disorders: Posterior Reversible Encephalopathy Syndrome (PRES).
Respiratory, thoracic and mediastinal disorders: Interstitial pneumonia, eosinophilic pneumonia and cryptogenic organizing pneumonia.
Skin reactions: Pustular psoriasis, erythrodermic psoriasis, hypersensitivity vasculitis.
Drug Interactions for Pyzchiva
Concomitant Therapies
In plaque psoriasis trials the safety of ustekinumab products in combination with immunosuppressive agents or phototherapy has not been evaluated. In psoriatic arthritis trials, concomitant MTX use did not appear to influence the safety or efficacy of ustekinumab. In Crohn's disease and ulcerative colitis induction trials, immunomodulators (6-MP, AZA, MTX) were used concomitantly in approximately 30% of subjects and corticosteroids were used concomitantly in approximately 40% and 50% of Crohn's disease and ulcerative colitis subjects, respectively. Use of these concomitant therapies did not appear to influence the overall safety or efficacy of ustekinumab.
CYP450 Substrates
The formation of CYP450 enzymes can be altered by increased levels of certain cytokines (e.g., IL-1, IL-6, IL-10, TNFα, IFN) during chronic inflammation. Thus, ustekinumab products, antagonists of IL12 and IL-23, could normalize the formation of CYP450 enzymes. Upon initiation of PYZCHIVA in patients who are receiving concomitant CYP450 substrates, particularly those with a narrow therapeutic index, consider monitoring for therapeutic effect (e.g., for warfarin) or drug concentration (e.g., for cyclosporine) and adjust the individual dose of the drug as needed [see CLINICAL PHARMACOLOGY].
Allergen Immunotherapy
Ustekinumab products have not been evaluated in patients who have undergone allergy immunotherapy. Ustekinumab products may decrease the protective effect of allergen immunotherapy (decrease tolerance) which may increase the risk of an allergic reaction to a dose of allergen immunotherapy. Therefore, caution should be exercised in patients receiving or who have received allergen immunotherapy, particularly for anaphylaxis.
Warnings for Pyzchiva
Included as part of the PRECAUTIONS section.
Precautions for Pyzchiva
Infections
Ustekinumab products may increase the risk of infections and reactivation of latent infections. Serious bacterial, mycobacterial, fungal, and viral infections were observed in patients receiving ustekinumab products [see ADVERSE REACTIONS].
Serious infections requiring hospitalization, or otherwise clinically significant infections, reported in clinical trials included the following:
- Plaque Psoriasis: diverticulitis, cellulitis, pneumonia, appendicitis, cholecystitis, sepsis, osteomyelitis, viral infections, gastroenteritis and urinary tract infections.
- Psoriatic arthritis: cholecystitis.
- Crohn's disease: anal abscess, gastroenteritis, ophthalmic herpes zoster, pneumonia, and listeria meningitis.
- Ulcerative colitis: gastroenteritis, ophthalmic herpes zoster, pneumonia, and listeriosis.
Avoid initiating treatment with PYZCHIVA in patients with any clinically important active infection until the infection resolves or is adequately treated. Consider the risks and benefits of treatment prior to initiating use of PYZCHIVA in patients with a chronic infection or a history of recurrent infection.
Instruct patients to seek medical advice if signs or symptoms suggestive of an infection occur while on treatment with PYZCHIVA and discontinue PYZCHIVA for serious or clinically significant infections until the infection resolves or is adequately treated.
Theoretical Risk For Vulnerability To Particular Infections
Individuals genetically deficient in IL-12/IL-23 are particularly vulnerable to disseminated infections from mycobacteria (including nontuberculous, environmental mycobacteria), salmonella (including nontyphi strains), and Bacillus Calmette-Guerin (BCG) vaccinations. Serious infections and fatal outcomes have been reported in such patients.
It is not known whether patients with pharmacologic blockade of IL-12/IL-23 from treatment with ustekinumab products may be susceptible to these types of infections. Consider appropriate diagnostic testing (e.g., tissue culture, stool culture, as dictated by clinical circumstances).
Pre-treatment Evaluation For Tuberculosis
Evaluate patients for tuberculosis infection prior to initiating treatment with PYZCHIVA.
Avoid administering PYZCHIVA to patients with active tuberculosis infection. Initiate treatment of latent tuberculosis prior to administering PYZCHIVA. Consider anti-tuberculosis therapy prior to initiation of PYZCHIVA in patients with a past history of latent or active tuberculosis in whom an adequate course of treatment cannot be confirmed. Closely monitor patients receiving PYZCHIVA for signs and symptoms of active tuberculosis during and after treatment.
Malignancies
Ustekinumab products are immunosuppressants and may increase the risk of malignancy. Malignancies were reported among subjects who received ustekinumab in clinical trials [see ADVERSE REACTIONS]. In rodent models, inhibition of IL-12/IL-23p40 increased the risk of malignancy [see Nonclinical Toxicology].
The safety of ustekinumab products has not been evaluated in patients who have a history of malignancy or who have a known malignancy.
There have been post-marketing reports of the rapid appearance of multiple cutaneous squamous cell carcinomas in patients receiving ustekinumab products who had pre-existing risk factors for developing non-melanoma skin cancer. Monitor all patients receiving PYZCHIVA for the appearance of non-melanoma skin cancer. Closely follow patients greater than 60 years of age, those with a medical history of prolonged immunosuppressant therapy and those with a history of PUVA treatment [see ADVERSE REACTIONS].
Hypersensitivity Reactions
Hypersensitivity reactions, including anaphylaxis and angioedema, have been reported with ustekinumab products [see ADVERSE REACTIONS]. If an anaphylactic or other clinically significant hypersensitivity reaction occurs, institute appropriate therapy and discontinue PYZCHIVA.
Posterior Reversible Encephalopathy Syndrome (PRES)
Two cases of posterior reversible encephalopathy syndrome (PRES), also known as Reversible Posterior Leukoencephalopathy Syndrome (RPLS), were reported in clinical trials. Cases have also been reported in postmarketing experience in patients with psoriasis, psoriatic arthritis and Crohn's disease. Clinical presentation included headaches, seizures, confusion, visual disturbances, and imaging changes consistent with PRES a few days to several months after ustekinumab product initiation. A few cases reported latency of a year or longer. Patients recovered with supportive care following withdrawal of ustekinumab products.
Monitor all patients treated with PYZCHIVA for signs and symptoms of PRES. If PRES is suspected, promptly administer appropriate treatment and discontinue PYZCHIVA.
Immunizations
Prior to initiating therapy with PYZCHIVA, patients should receive all age-appropriate immunizations as recommended by current immunization guidelines. Patients being treated with PYZCHIVA should avoid receiving live vaccines. Avoid administering BCG vaccines during treatment with PYZCHIVA or for one year prior to initiating treatment or one year following discontinuation of treatment. Caution is advised when administering live vaccines to household contacts of patients receiving PYZCHIVA because of the potential risk for shedding from the household contact and transmission to patient.
Non-live vaccinations received during a course of PYZCHIVA may not elicit an immune response sufficient to prevent disease.
Noninfectious Pneumonia
Cases of interstitial pneumonia, eosinophilic pneumonia and cryptogenic organizing pneumonia have been reported during post-approval use of ustekinumab products. Clinical presentations included cough, dyspnea, and interstitial infiltrates following one to three doses. Serious outcomes have included respiratory failure and prolonged hospitalization. Patients improved with discontinuation of therapy and in certain cases administration of corticosteroids. If diagnosis is confirmed, discontinue PYZCHIVA and institute appropriate treatment [see ADVERSE REACTIONS].
Patient Counseling Information
Advise the patient and/or caregiver to read the FDA-approved patient labeling (Medication Guide and Instructions for Use).
Infections
Inform patients that PYZCHIVA may lower the ability of their immune system to fight infections and to contact their healthcare provider immediately if they develop any signs or symptoms of infection [see WARNINGS AND PRECAUTIONS].
Malignancies
Inform patients of the risk of developing malignancies while receiving PYZCHIVA [see WARNINGS AND PRECAUTIONS].
Hypersensitivity Reactions
- Advise patients to seek immediate medical attention if they experience any signs or symptoms of serious hypersensitivity reactions and discontinue PYZCHIVA [see WARNINGS AND PRECAUTIONS].
Posterior Reversible Encephalopathy Syndrome (PRES)
Inform patients to immediately contact their healthcare provider if they experience signs and symptoms of PRES (which may include headache, seizures, confusion, or visual disturbances) [see WARNINGS AND PRECAUTIONS].
Immunizations
Inform patients that PYZCHIVA can interfere with the usual response to immunizations and that they should avoid live vaccines [see WARNINGS AND PRECAUTIONS].
Administration
Instruct patients to follow sharps disposal recommendations, as described in the Instructions for Use.
Nonclinical Toxicology
Carcinogenesis, Mutagenesis, Impairment Of Fertility
Animal studies have not been conducted to evaluate the carcinogenic or mutagenic potential of ustekinumab products. Published literature showed that administration of murine IL-12 caused an anti-tumor effect in mice that contained transplanted tumors and IL-12/IL-23p40 knockout mice or mice treated with anti-IL-12/IL-23p40 antibody had decreased host defense to tumors. Mice genetically manipulated to be deficient in both IL-12 and IL-23 or IL-12 alone developed UV-induced skin cancers earlier and more frequently compared to wild-type mice. The relevance of these experimental findings in mouse models for malignancy risk in humans is unknown.
No effects on fertility were observed in male cynomolgus monkeys that were administered ustekinumab at subcutaneous doses up to 45 mg/kg twice weekly (45 times the MRHD on a mg/kg basis) prior to and during the mating period. However, fertility and pregnancy outcomes were not evaluated in mated females.
No effects on fertility were observed in female mice that were administered an analogous IL-12/ILÂ23p40 antibody by subcutaneous administration at doses up to 50 mg/kg, twice weekly, prior to and during early pregnancy.
Use In Specific Populations
Pregnancy
Risk Summary
Limited data from observational studies, published case reports, and postmarketing surveillance on the use of ustekinumab products during pregnancy are insufficient to inform a drug associated risk of major birth defects, miscarriage, and other adverse maternal or fetal outcomes. Transport of human IgG antibody across the placenta increases as pregnancy progresses and peaks during the third trimester; therefore, ustekinumab products may be transferred to the developing fetus (see Clinical Considerations). In animal reproductive and developmental toxicity studies, no adverse developmental effects were observed in offspring after administration of ustekinumab to pregnant monkeys at exposures greater than 100 times the maximum recommended human dose (MRHD).
The background risk of major birth defects and miscarriage for the indicated population(s) are unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage of clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Clinical Considerations
Fetal/Neonatal Adverse Reactions
Because ustekinumab products may theoretically interfere with immune response to infections, consider risks and benefits prior to administering live vaccines to infants exposed to PYZCHIVA in utero. There are insufficient data regarding exposed infant serum levels of ustekinumab products at birth and the duration of persistence of ustekinumab products in infant serum after birth. Although a specific timeframe to delay administration of live attenuated vaccines in infants exposed in utero is unknown, consider the risks and benefits of delaying a minimum of 6 months after birth because of the clearance of the product.
Data
Animal Data
Ustekinumab was tested in two embryo-fetal development toxicity studies in cynomolgus monkeys. No teratogenic or other adverse developmental effects were observed in fetuses from pregnant monkeys that were administered ustekinumab subcutaneously twice weekly or intravenously weekly during the period of organogenesis. Serum concentrations of ustekinumab in pregnant monkeys were greater than 100 times the serum concentration in patients treated subcutaneously with 90 mg of ustekinumab weekly for 4 weeks.
In a combined embryo-fetal development and pre-and post-natal development toxicity study, pregnant cynomolgus monkeys were administered subcutaneous doses of ustekinumab twice weekly at exposures greater than 100 times the MRHD from the beginning of organogenesis to Day 33 after delivery. Neonatal deaths occurred in the offspring of one monkey administered ustekinumab at 22.5 mg/kg and one monkey dosed at 45 mg/kg. No ustekinumab-related effects on functional, morphological, or immunological development were observed in the neonates from birth through six months of age.
Lactation
Risk Summary
Limited data from published literature suggests that ustekinumab is present in human breast milk. There are no available data on the effects of ustekinumab products on milk production. The effects of local gastrointestinal exposure and limited systemic exposure in the breastfed infant to ustekinumab products are unknown. No adverse effects on the breastfed infant causally related to ustekinumab products have been identified in the published literature or postmarketing experience.
The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for PYZCHIVA and any potential adverse effects on the breastfed child from PYZCHIVA or from the underlying maternal condition.
Pediatric Use
Plaque Psoriasis
The safety and effectiveness of PYZCHIVA have been established for the treatment of moderate to severe plaque psoriasis in pediatric patients 6 to 17 years of age who are candidates for phototherapy or systemic therapy.
Use of PYZCHIVA in pediatric patients 12 to less than 17 years of age is supported by evidence from a multicenter, randomized, 60 week trial (Ps STUDY 3) of ustekinumab that included a 12 week, double-blind, placebo-controlled, parallel group portion, in 110 pediatric subjects 12 years of age and older [see ADVERSE REACTIONS, Clinical Studies].
Use of PYZCHIVA in pediatric patients 6 to 11 years of age is supported by evidence from an open-label, single-arm, efficacy, safety and pharmacokinetics trial (Ps STUDY 4) of ustekinumab in 44 subjects [see ADVERSE REACTIONS, CLINICAL PHARMACOLOGY].
The safety and effectiveness of PYZCHIVA have not been established in pediatric patients less than 6 years of age with plaque psoriasis.
Psoriatic Arthritis
The safety and effectiveness of PYZCHIVA have been established for treatment of psoriatic arthritis in pediatric patients 6 to 17 years old.
Use of PYZCHIVA in these age groups is supported by evidence from adequate and well controlled trials of ustekinumab in adults with psoriasis and PsA, pharmacokinetic data from adult patients with psoriasis, adult patients with PsA and pediatric patients with psoriasis, and safety data of ustekinumab from two clinical trials in 44 pediatric patients 6 to 11 years old with psoriasis and 110 pediatric patients 12 to 17 years old with psoriasis. The observed pre-dose (trough) concentrations are generally comparable between adult patients with psoriasis, adult patients with PsA and pediatric patients with psoriasis, and the PK exposure is expected to be comparable between adult and pediatric patients with PsA [see ADVERSE REACTIONS, CLINICAL PHARMACOLOGY, and Clinical Studies].
The safety and effectiveness of PYZCHIVA have not been established in pediatric patients less than 6 years old with psoriatic arthritis.
Crohn's Disease And Ulcerative Colitis
The safety and effectiveness of PYZCHIVA have not been established in pediatric patients with Crohn's disease or ulcerative colitis.
Geriatric Use
Of the 6709 patients exposed to ustekinumab, a total of 340 were 65 years of age or older (183 patients with plaque psoriasis, 65 patients with psoriatic arthritis, 58 patients with Crohn's disease and 34 patients with ulcerative colitis), and 40 patients were 75 years of age or older. Clinical trials of ustekinumab did not include sufficient numbers of patients 65 years of age and older to determine whether they respond differently from younger adult patients.
REFERENCES
1 Surveillance, Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov) SEER*Stat Database: Incidence -SEER 6.6.2 Regs Research Data, Nov 2009 Sub (1973–2007) ÂLinked To County Attributes -Total U.S., 1969– 2007 Counties, National Cancer Institute, DCCPS, Surveillance Research Program, Surveillance Systems Branch, released April 2010, based on the November 2009 submission.
Overdose Information for Pyzchiva
Single doses up to 6 mg/kg intravenously have been administered in clinical trials without dose-limiting toxicity. In case of overdosage, monitor the patient for any signs or symptoms of adverse reactions or effects and institute appropriate symptomatic treatment immediately. Consider contacting the Poison Help line (1-800-222-1222) or a medical toxicologist for additional overdose management recommendations.
Contraindications for Pyzchiva
PYZCHIVA is contraindicated in patients with clinically significant hypersensitivity to ustekinumab products or to any of the excipients in PYZCHIVA [see WARNINGS AND PRECAUTIONS].
Clinical Pharmacology for Pyzchiva
Mechanism Of Action
Ustekinumab products are human IgG1κ monoclonal antibodies that bind with specificity to the p40 protein subunit used by both the IL-12 and IL-23 cytokines. IL-12 and IL-23 are naturally occurring cytokines that are involved in inflammatory and immune responses, such as natural killer cell activation and CD4+ T-cell differentiation and activation. In in vitro models, ustekinumab products were shown to disrupt IL-12 and IL-23 mediated signaling and cytokine cascades by disrupting the interaction of these cytokines with a shared cell-surface receptor chain, IL-12Rβ1. The cytokines IL-12 and IL-23 have been implicated as important contributors to the chronic inflammation that is a hallmark of Crohn's disease and ulcerative colitis. In animal models of colitis, genetic absence or antibody blockade of the p40 subunit of IL-12 and IL-23, the target of ustekinumab products, was shown to be protective.
Pharmacodynamics
Plaque Psoriasis
In a small exploratory trial, a decrease was observed in the expression of mRNA of its molecular targets IL-12 and IL-23 in lesional skin biopsies measured at baseline and up to two weeks post-treatment in subjects with plaque psoriasis.
Ulcerative Colitis
In both trial UC-1 (induction) and trial UC-2 (maintenance), a positive relationship was observed between exposure and rates of clinical remission, clinical response, and endoscopic improvement. The response rate approached a plateau at the ustekinumab exposures associated with the recommended dosing regimen for maintenance treatment [see Clinical Studies].
Pharmacokinetics
Absorption
In adult subjects with plaque psoriasis, the median time to reach the maximum serum concentration (Tmax) was 13.5 days and 7 days, respectively, after a single subcutaneous administration of 45 mg (N=22) and 90 mg (N=24) of ustekinumab. In healthy subjects (N=30), the median Tmax value (8.5 days) following a single subcutaneous administration of 90 mg of ustekinumab was comparable to that observed in subjects with plaque psoriasis.
Following multiple subcutaneous doses of ustekinumab in adult subjects with plaque psoriasis, steady-state serum concentrations of ustekinumab were achieved by Week 28. The mean (±SD) steady-state trough serum ustekinumab concentrations were 0.69 ± 0.69 mcg/mL for patients less than or equal to 100 kg receiving a 45 mg dose and 0.74 ± 0.78 mcg/mL for patients greater than 100 kg receiving a 90 mg dose. There was no apparent accumulation in serum ustekinumab concentration over time when given subcutaneously every 12 weeks.
Following the recommended intravenous induction dose, mean ±SD peak serum ustekinumab concentration was 125.2 ± 33.6 mcg/mL in patients with Crohn's disease, and 129.1 ± 27.6 mcg/mL in patients with ulcerative colitis. Starting at Week 8, the recommended subcutaneous maintenance dosing of 90 mg ustekinumab was administered every 8 weeks. Steady state ustekinumab concentration was achieved by the start of the second maintenance dose. There was no apparent accumulation in ustekinumab concentration over time when given subcutaneously every 8 weeks. Mean ± SD steady-state trough concentration was 2.5 ± 2.1 mcg/mL in patients with Crohn's disease, and 3.3 ± 2.3 mcg/mL in patients with ulcerative colitis for 90 mg ustekinumab administered every 8 weeks.
Distribution
Population pharmacokinetic analyses showed that the volume of distribution of ustekinumab in the central compartment was 2.7 L (95% CI: 2.69, 2.78) in patients with Crohn's disease and 3.0 L (95% CI: 2.96, 3.07) in patients with ulcerative colitis. The total volume of distribution at steady-state was 4.6 L in patients with Crohn's disease and 4.4 L in patients with ulcerative colitis.
Elimination
The mean (±SD) half-life ranged from 14.9 ± 4.6 to 45.6 ± 80.2 days across all plaque psoriasis trials following subcutaneous administration. Population pharmacokinetic analyses showed that the clearance of ustekinumab was 0.19 L/day (95% CI: 0.185, 0.197) in patients with Crohn's disease and 0.19 L/day  (95% CI: 0.179, 0.192) in patients with ulcerative colitis with an estimated median terminal half-life of approximately 19 days for both IBD (Crohn's disease and ulcerative colitis) populations.
These results indicate the pharmacokinetics of ustekinumab were similar between patients with Crohn's disease and ulcerative colitis.
Metabolism
The metabolic pathway of ustekinumab products has not been characterized. As a human IgG1κ monoclonal antibody, ustekinumab products are expected to be degraded into small peptides and amino acids via catabolic pathways in the same manner as endogenous IgG.
Specific Populations
Weight
When given the same dose, subjects with plaque psoriasis or psoriatic arthritis weighing more than 100 kg had lower median serum ustekinumab concentrations compared with those subjects weighing 100 kg or less. The median trough serum concentrations of ustekinumab in subjects of higher weight (greater than 100 kg) in the 90 mg group were comparable to those in subjects of lower weight (100 kg or less) in the 45 mg group.
Age: Geriatric Population
A population pharmacokinetic analysis (N=106/1937 patients with plaque psoriasis greater than or equal to 65 years old) was performed to evaluate the effect of age on the pharmacokinetics of ustekinumab. There were no apparent changes in pharmacokinetic parameters (clearance and volume of distribution) in subjects older than 65 years old.
Age: Pediatric Population
Following multiple recommended doses of ustekinumab in pediatric subjects 6 to 17 years of age with plaque psoriasis, steady-state serum concentrations of ustekinumab were achieved by Week 28. At Week 28, the mean ±SD steady-state trough serum ustekinumab concentrations were 0.36 ± 0.26 mcg/mL and 0.54 ± 0.43 mcg/mL, respectively, in pediatric subjects 6 to 11 years of age and pediatric subjects 12 to 17 years of age.
Overall, the observed steady-state ustekinumab trough concentrations in pediatric patients with plaque psoriasis were within the range of those observed for adult patients with plaque psoriasis and adult patients with PsA after administration of ustekinumab.
Drug Interaction Studies
The effects of IL-12 or IL-23 on the regulation of CYP450 enzymes were evaluated in an in vitro study using human hepatocytes, which showed that IL-12 and/or IL-23 at levels of 10 ng/mL did not alter human CYP450 enzyme activities (CYP1A2, 2B6, 2C9, 2C19, 2D6, or 3A4). However, the clinical relevance of in vitro data has not been established [see DRUG INTERACTIONS].
No in vivo drug interaction studies have been conducted with ustekinumab products.
Population pharmacokinetic analyses indicated that the clearance of ustekinumab was not impacted by concomitant MTX, NSAIDs, and oral corticosteroids, or prior exposure to a TNF blocker in patients with psoriatic arthritis.
In patients with Crohn's disease and ulcerative colitis, population pharmacokinetic analyses did not indicate changes in ustekinumab clearance with concomitant use of corticosteroids or immunomodulators (AZA, 6-MP, or MTX); and serum ustekinumab concentrations were not impacted by concomitant use of these medications.
Animal Toxicology And/Or Pharmacology
In a 26-week toxicology study, one out of 10 monkeys subcutaneously administered 45 mg/kg ustekinumab twice weekly for 26 weeks had a bacterial infection.
Clinical Studies
Adult Plaque Psoriasis
Two multicenter, randomized, double-blind, placebo-controlled trials (Ps STUDY 1 and Ps STUDY 2) enrolled a total of 1996 subjects 18 years of age and older with plaque psoriasis who had a minimum body surface area involvement of 10%, and Psoriasis Area and Severity Index (PASI) score ≥12, and who were candidates for phototherapy or systemic therapy. Subjects with guttate, erythrodermic, or pustular psoriasis were excluded from the trials.
Ps STUDY 1 enrolled 766 subjects and Ps STUDY 2 enrolled 1230 subjects. The trials had the same design through Week 28. In both trials, subjects were randomized in equal proportion to placebo, 45 mg or 90 mg of ustekinumab. Subjects randomized to ustekinumab received 45 mg or 90 mg doses, regardless of weight, at Weeks 0, 4, and 16. Subjects randomized to receive placebo at Weeks 0 and 4 crossed over to receive ustekinumab (either 45 mg or 90 mg) at Weeks 12 and 16.
In both trials, subjects in all treatment groups had a median baseline PASI score ranging from approximately 17 to 18. Baseline PGA score was marked or severe in 44% of subjects in Ps STUDY 1 and 40% of subjects in Ps STUDY 2. Approximately two-thirds of all subjects had received prior phototherapy, 69% had received either prior conventional systemic or biologic therapy for the treatment of psoriasis, with 56% receiving prior conventional systemic therapy and 43% receiving prior biologic therapy. A total of 28% of subjects had a history of psoriatic arthritis.
In both trials, the endpoints were the proportion of subjects who achieved at least a 75% reduction in PASI score (PASI 75) from baseline to Week 12 and treatment success (cleared or minimal) on the Physician's Global Assessment (PGA). The PGA is a 6-category scale ranging from 0 (cleared) to 5 (severe) that indicates the physician's overall assessment of psoriasis focusing on plaque thickness/induration, erythema, and scaling.
Clinical Response
The results of Ps STUDY 1 and Ps STUDY 2 are presented in Table 7 below.
Table 7: Clinical Outcomes at Week 12 in Adults with Plaque Psoriasis in Ps STUDY 1 and Ps STUDY 2
| Placebo | Ps STUDY 1 Ustekinumab 45 mg | 90 mg | Placebo | Ps STUDY 2 Ustekinumab 45 mg | 90 mg | |
| Subjects randomized | 255 | 255 | 256 | 410 | 409 | 411 |
| PASI 75 response | 8 (3%) | 171 (67%) | 170 (66%) | 15 (4%) | 273 (67%) | 311 (76%) |
| PGA of Cleared or Minimal | 10 (4%) | 151 (59%) | 156 (61%) | 18 (4%) | 277 (68%) | 300 (73%) |
Examination of age, gender, and race subgroups did not identify differences in response to ustekinumab among these subgroups.
In subjects who weighed 100 kg or less, response rates were comparable with both the 45 mg and 90 mg doses; however, in subjects who weighed greater than 100 kg, higher response rates were seen with 90 mg dosing compared with 45 mg dosing (Table 8 below).
Table 8: Clinical Outcomes by Weight at Week 12 in Adults with Plaque Psoriasis in Ps STUDY 1 and Ps STUDY 2
| Placebo | Ps STUDY 1 Ustekinumab | Placebo | Ps STUDY 2 | |||
| 45 mg | 90 mg | Ustekinumab 45 mg | 90 mg | |||
| Subjects randomized | 255 | 255 | 256 | 410 | 409 | 411 |
| PASI 75 response* | ||||||
| ≤100 kg | 4% | 74% | 65% | 4% | 73% | 78% |
| 6/166 | 124/168 | 107/164 | 12/290 | 218/297 | 225/289 | |
| >100 kg | 2% | 54% | 68% | 3% | 49% | 71% |
| 2/89 | 47/87 | 63/92 | 3/120 | 55/112 | 86/121 | |
| PGA of Cleared or Minimal * | ||||||
| ≤100 kg | 4% | 64% | 63% | 5% | 74% | 75% |
| 7/166 | 108/168 | 103/164 | 14/290 | 220/297 | 216/289 | |
| >100 kg | 3% | 49% | 58% | 3% | 51% | 69% |
| 3/89 | 43/87 | 53/92 | 4/120 | 57/112 | 84/121 | |
| * Patients were dosed with trial medication at Weeks 0 and 4. | ||||||
Subjects in Ps STUDY 1 who were PASI 75 responders at both Weeks 28 and 40 were re-randomized at Week 40 to either continued dosing of ustekinumab (ustekinumab at Week 40) or to withdrawal of therapy (placebo at Week 40). At Week 52, 89% (144/162) of subjects re-randomized to ustekinumab treatment were PASI 75 responders compared with 63% (100/159) of subjects re-randomized to placebo (treatment withdrawal after Week 28 dose). The median time to loss of PASI 75 response among the subjects randomized to treatment withdrawal was 16 weeks.
Pediatric Plaque Psoriasis
A multicenter, randomized, double blind, placebo-controlled trial (Ps STUDY 3) enrolled 110 pediatric subjects 12 to 17 years of age with a minimum BSA involvement of 10%, a PASI score greater than or equal to 12, and a PGA score greater than or equal to 3, who were candidates for phototherapy or systemic therapy and whose disease was inadequately controlled by topical therapy.
Subjects were randomized to receive placebo (n = 37), the recommended dose of ustekinumab (n = 36), or one-half the recommended dose of ustekinumab (n = 37) by subcutaneous injection at Weeks 0 and 4 followed by dosing every 12 weeks (q12w). The recommended dose of ustekinumab was 0.75 mg/kg for subjects weighing less than 60 kg, 45 mg for subjects weighing 60 kg to 100 kg, and 90 mg for subjects weighing greater than 100 kg. At Week 12, subjects who received placebo were crossed over to receive ustekinumab at the recommended dose or one-half the recommended dose.
Of the pediatric subjects, approximately 63% had prior exposure to phototherapy or conventional systemic therapy and approximately 11% had prior exposure to biologics.
The endpoints were the proportion of subjects who achieved a PGA score of cleared (0) or minimal (1), PASI 75, and PASI 90 at Week 12. Subjects were followed for up to 60 weeks following first administration of trial agent.
Clinical Response
The efficacy results at Week 12 for Ps STUDY 3 are presented in Table 9.
Table 9: Efficacy Results at Week 12 in Pediatric Subjects 12 to 17 years with Plaque Psoriasis in Ps STUDY 3
| Ps STUDY 3 | ||
| Placebo n (%) | Ustekinumab* n (%) | |
| N | 37 | 36 |
| PGA | ||
| PGA of cleared (0) or minimal (1) | 2 (5.4%) | 25 (69.4%) |
| PASI | ||
| PASI 75 responders | 4 (10.8%) | 29 (80.6%) |
| PASI 90 responders | 2 (5.4%) | 22 (61.1%) |
| * Using the weight-based dosage regimen specified in Table 1. | ||
Psoriatic Arthritis
The safety and efficacy of ustekinumab was assessed in 927 patients (PsA STUDY 1, n=615; PsA STUDY 2, n=312), in two randomized, double-blind, placebo-controlled trials in adult patients 18 years of age and older with active PsA (≥5 swollen joints and ≥5 tender joints) despite nonsteroidal anti-inflammatory (NSAID) or disease modifying antirheumatic (DMARD) therapy. Patients in these trials had a diagnosis of PsA for at least 6 months. Patients with each subtype of PsA were enrolled, including polyarticular arthritis with the absence of rheumatoid nodules (39%), spondylitis with peripheral arthritis (28%), asymmetric peripheral arthritis (21%), distal interphalangeal involvement (12%) and arthritis mutilans (0.5%). Over 70% and 40% of the patients, respectively, had enthesitis and dactylitis at baseline.
Patients were randomized to receive treatment with ustekinumab 45 mg, 90 mg, or placebo subcutaneously at Weeks 0 and 4 followed by every 12 weeks (q12w) dosing. Approximately 50% of patients continued on stable doses of MTX (≤25 mg/week). The primary endpoint was the percentage of patients achieving ACR 20 response at Week 24.
In PsA STUDY 1 and PsA STUDY 2, 80% and 86% of the patients, respectively, had been previously treated with DMARDs. In PsA STUDY 1, previous treatment with anti-tumor necrosis factor (TNF)-α agent was not allowed. In PsA STUDY 2, 58% (n=180) of the patients had been previously treated with TNF blocker, of whom over 70% had discontinued their TNF blocker treatment for lack of efficacy or intolerance at any time.
Clinical Response
In both trials, a greater proportion of patients achieved ACR 20, ACR 50 and PASI 75 response in the ustekinumab 45 mg and 90 mg groups compared to placebo at Week 24 (see Table 10). ACR 70 responses were also higher in the ustekinumab 45 mg and 90 mg groups, although the difference was only numerical (p=NS) in STUDY 2. Responses were consistent in patients treated with ustekinumab alone or in combination with methotrexate. Responses were similar in patients regardless of prior TNFα exposure.
Table 10: ACR 20, ACR 50, ACR 70 and PASI 75 responses in PsA STUDY 1 and PsA STUDY 2 at Week 24
| Placebo | PsA STUDY 1 Ustekinumab | Placebo | PsA STUDY 2 Ustekinumab | |||
| 45 mg | 90 mg | 45 mg | 90 mg | |||
| Number of patients | ||||||
| Randomized | 206 | 205 | 204 | 104 | 103 | 105 |
| ACR 20 response, N (%) | 47 (23%) | 87 (42%) | 101 (50%) | 21 (20%) | 45 (44%) | 46 (44%) |
| ACR 50 response, N (%) | 18 (9%) | 51 (25%) | 57 (28%) | 7 (7%) | 18 (17%) | 24 (23%) |
| ACR 70 response, N (%) | 5 (2%) | 25 (12%) | 29 (14%) | 3 (3%) | 7 (7%) | 9 (9%) |
| Number of patients with ≥ 3% BSA* | 146 | 145 | 149 | 80 | 80 | 81 |
| PASI 75 response, N (%) | 16 (11%) | 83 (57%) | 93 (62%) | 4 (5%) | 41 (51%) | 45 (56%) |
| *Number of patients with ≥ 3% BSA psoriasis skin involvement at baseline | ||||||
The percent of patients achieving ACR 20 responses by visit is shown in Figure 1.
Figure 1: Percent of patients achieving ACR 20 response through Week 24
 |
The results of the components of the ACR response criteria are shown in Table 11.
Table 11: Mean change from baseline in ACR components at Week 24
| PsA STUDY 1 | |||
| Placebo (N = 206) |
Ustekinumab | ||
| 45 mg (N = 205) |
90 mg (N = 204) |
||
| Number of swollen jointsa | |||
| Baseline | 15 | 12 | 13 |
| Mean Change at Week 24 | -3 | -5 | -6 |
| Number of tender jointsb | |||
| Baseline | 25 | 22 | 23 |
| Mean Change at Week 24 | -4 | -8 | -9 |
| Patient's assessment of painc | |||
| Baseline | 6.1 | 6.2 | 6.6 |
| Mean Change at Week 24 | -0.5 | -2.0 | -2.6 |
| Patient global assessmentc | |||
| Baseline | 6.1 | 6.3 | 6.4 |
| Mean Change at Week 24 | -0.5 | -2.0 | -2.5 |
| Physician global assessmentc | |||
| Baseline | 5.8 | 5.7 | 6.1 |
| Mean Change at Week 24 | -1.4 | -2.6 | -3.1 |
| Disability index (HAQ)d | |||
| Baseline | 1.2 | 1.2 | 1.2 |
| Mean Change at Week 24 | -0.1 | -0.3 | -0.4 |
| CRP (mg/dL)e | |||
| Baseline | 1.6 | 1.7 | 1.8 |
| Mean Change at Week 24 | 0.01 | -0.5 | -0.8 |
| a Number of swollen joints counted (0–66) b Number of tender joints counted (0–68) c Visual analogue scale; 0= best, 10=worst. d Disability Index of the Health Assessment Questionnaire; 0 = best, 3 = worst, measures the patient's ability to perform the following: dress/groom, arise, eat, walk, reach, grip, maintain hygiene, and maintain daily activity. e CRP: (Normal Range 0.0–1.0 mg/dL) |
|||
An improvement in enthesitis and dactylitis scores was observed in each ustekinumab group compared with placebo at Week 24.
Physical Function
Ustekinumab-treated patients showed improvement in physical function compared to patients treated with placebo as assessed by HAQ-DI at Week 24. In both trials, the proportion of HAQ-DI responders (≥0.3 improvement in HAQ-DI score) was greater in the ustekinumab 45 mg and 90 mg groups compared to placebo at Week 24.
Crohn's Disease
Ustekinumab was evaluated in three randomized, double-blind, placebo-controlled clinical trials in adult patients with moderately to severely active Crohn's disease (Crohn's Disease Activity Index [CDAI] score of 220 to 450). There were two 8-week intravenous induction trials (CD-1 and CD-2) followed by a 44-week subcutaneous randomized withdrawal maintenance trial (CD-3) representing 52 weeks of therapy. Patients in CD-1 had failed or were intolerant to treatment with one or more TNF blockers, while patients in CD-2 had failed or were intolerant to treatment with immunomodulators or corticosteroids, but never failed treatment with a TNF blocker.
Trials CD-1 And CD-2
In trials CD-1 and CD-2, 1409 patients were randomized, of whom 1368 (CD-1, n=741; CD-2, n=627) were included in the final efficacy analysis. Induction of clinical response (defined as a reduction in CDAI score of greater than or equal to 100 points or CDAI score of less than 150) at Week 6 and clinical remission (defined as a CDAI score of less than 150) at Week 8 were evaluated. In both trials, patients were randomized to receive a single intravenous administration of ustekinumab at either approximately 6 mg/kg, placebo (see Table 3), or 130 mg (a lower dose than recommended).
In trial CD-1, patients had failed or were intolerant to prior treatment with a TNF blocker: 29% patients had an inadequate initial response (primary non-responders), 69% responded but subsequently lost response (secondary non-responders) and 36% were intolerant to a TNF blocker. Of these patients, 48% failed or were intolerant to one TNF blocker and 52% had failed 2 or 3 prior TNF blockers. At baseline and throughout the trial, approximately 46% of the patients were receiving corticosteroids and 31% of the patients were receiving immunomodulators (AZA, 6-MP, MTX). The median baseline CDAI score was 319 in the ustekinumab approximately 6 mg/kg group and 313 in the placebo group.
In trial CD-2, patients had failed or were intolerant to prior treatment with corticosteroids (81% of patients), at least one immunomodulator (6-MP, AZA, MTX; 68% of patients), or both (49% of patients). Additionally, 69% never received a TNF blocker and 31% previously received but had not failed a TNF blocker. At baseline, and throughout the trial, approximately 39% of the patients were receiving corticosteroids and 35% of the patients were receiving immunomodulators (AZA, 6-MP, MTX). The median baseline CDAI score was 286 in the ustekinumab and 290 in the placebo group.
In these induction trials, a greater proportion of patients treated with ustekinumab (at the recommended dose of approximately 6 mg/kg dose) achieved clinical response at Week 6 and clinical remission at Week 8 compared to placebo (see Table 12 for clinical response and remission rates). Clinical response and remission were significant as early as Week 3 in ustekinumab-treated patients and continued to improve through Week 8.
Table 12: Induction of Clinical Response and Remission in CD-1* and CD-2**
| Placebo N = 247 |
CD-1 n = 741 |
Placebo N = 209 |
CD-2 n = 627 |
|||
| Ustekinumab†, N = 249 |
Treatment difference and 95% Cl | Ustekinumab† N = 209 |
Treatment difference and 95% Cl | |||
| Clinical Response (100 point), Week 6 | 53 (21%) | 84 (34%)a | 12% (4%, 20%) | 60 (29%) | 116 (56%)b | 27% (18%, 36%) |
| Clinical Remission,Week 8 | 18 (7%) | 52 (21%)b | 14%(8%, 20%) | 41 (20%) | 84 (40%)b | 21%(12%, 29%) |
| Clinical Response (100 point), Week 8 | 50 (20%) | 94 (38%)b | 18%(10%, 25%) | 67 (32%) | 121 (58%)b | 26%(17%, 35%) |
| 70 Point Response, Week 6 | 75 (30%) | 109 (44%)a | 13% (5%, 22%) | 81 (39%) | 135 (65%)b | 26% (17%, 35%) |
| 70 Point Response, Week 3 | 67 (27%) | 101 (41%)a | 13% (5%, 22%) | 66 (32%) | 106 (51%)b | 19% (10%, 28%) |
| Clinical remission is defined as CDAI score < 150; Clinical response is defined as reduction in CDAI score by at least 100 points or being in clinical remission: 70 point response is defined as reduction in CDAI score by at least 70 points * Patient population consisted of patients who failed or were intolerant to TNF blocker therapy ** Patient population consisted of patients who failed or were intolerant to corticosteroids or immunomodulators (e.g., 6-MP, AZA, MTX) and previously received but not failed a TNF blocker or were never treated with a TNF blocker. † Infusion dose of ustekinumab using the weight-based dosage regimen specified in Table 3. a 0.001≤ p < 0.01 b p < 0.001 |
||||||
Trial CD-3
The maintenance trial (CD-3), evaluated 388 patients who achieved clinical response (≥ 100 point reduction in CDAI score) at Week 8 with either induction dose of ustekinumab in trials CD-1 or CD-2. Patients were randomized to receive a subcutaneous maintenance regimen of either 90 mg ustekinumab every 8 weeks or placebo for 44 weeks (see Table 13).
Table 13: Clinical Response and Remission in CD-3 (Week 44; 52 weeks from initiation of the induction dose)
| Placebo* N = 131** |
90 mg ustekinumab every 8 weeks N = 128** |
Treatment difference and 95% CI | |
| Clinical Remission | 47 (36%) | 68 (53%)† | 17% (5%, 29%) |
| Clinical Response | 58 (44%) | 76 (59%)a | 15% (3%, 27%) |
| Clinical Remission in patients in remission at the start of maintenance therapyb | 36/79 (46%) | 52/78 (67%)† | 21% (6%, 36%) |
| Clinical remission is defined as CDAI score < 150; Clinical response is defined as reduction in CDAI of at least 100 points or being in clinical remission * The placebo group consisted of patients who were in response to ustekinumab and were randomized to receive placebo at the start of maintenance therapy. ** Patients who achieved clinical response to ustekinumab at the end of the induction trial. † p < 0.01 a 0.01≤ p < 0.05 b Patients in remission at the end of maintenance therapy who were in remission at the start of maintenance therapy. This does not account for any other time point during maintenance therapy. |
|||
At Week 44, 47% of patients who received ustekinumab were corticosteroid-free and in clinical remission, compared to 30% of patients in the placebo group.
At Week 0 of trial CD-3, 34/56 (61%) ustekinumab-treated patients who previously failed or were intolerant to TNF blocker therapies were in clinical remission and 23/56 (41%) of these patients were in clinical remission at Week 44. In the placebo arm, 27/61 (44%) patients were in clinical remission at Week 0 while 16/61 (26%) of these patients were in remission at Week 44.
At Week 0 of trial CD-3, 46/72 (64%) ustekinumab-treated patients who had previously failed immunomodulator therapy or corticosteroids (but not TNF blockers) were in clinical remission and 45/72 (63%) of these patients were in clinical remission at Week 44. In the placebo arm, 50/70 (71%) of these patients were in clinical remission at Week 0 while 31/70 (44%) were in remission at Week 44. In the subset of these patients who were also naïve to TNF blockers, 34/52 (65%) of ustekinumab-treated patients were in clinical remission at Week 44 as compared to 25/51 (49%) in the placebo arm.
Patients who were not in clinical response 8 weeks after ustekinumab induction were not included in the primary efficacy analyses for trial CD-3; however, these patients were eligible to receive a 90 mg subcutaneous injection of ustekinumab upon entry into trial CD-3. Of these patients, 102/219 (47%) achieved clinical response eight weeks later and were followed for the duration of the trial.
Ulcerative Colitis
Ustekinumab was evaluated in two randomized, double-blind, placebo-controlled clinical trials [UC-1 and UC-2 (NCT02407236)] in adult patients with moderately to severely active ulcerative colitis who had an inadequate response to or failed to tolerate a biologic (i.e., TNF blocker and/or vedolizumab), corticosteroids, and/or 6-MP or AZA therapy. The 8-week intravenous induction trial (UC-1) was followed by the 44-week subcutaneous randomized withdrawal maintenance trial (UC-2) for a total of 52 weeks of therapy.
Disease assessment was based on the Mayo score, which ranged from 0 to 12 and has four subscores that were each scored from 0 (normal) to 3 (most severe): stool frequency, rectal bleeding, findings on centrally-reviewed endoscopy, and physician global assessment. Moderately to severely active ulcerative colitis was defined at baseline (Week 0) as Mayo score of 6 to 12, including a Mayo endoscopy subscore ≥2. An endoscopy score of 2 was defined by marked erythema, absent vascular pattern, friability, erosions; and a score of 3 was defined by spontaneous bleeding, ulceration. At baseline, patients had a median Mayo score of 9, with 84% of patients having moderate disease (Mayo score 6–10) and 15% having severe disease (Mayo score 11–12).
Patients in these trials may have received other concomitant therapies including aminosalicylates, immunomodulatory agents (AZA, 6-MP, or MTX), and oral corticosteroids (prednisone).
Trial UC-1
In UC-1, 961 patients were randomized at Week 0 to a single intravenous administration of ustekinumab of approximately 6 mg/kg, 130 mg (a lower dose than recommended), or placebo. Patients enrolled in UC-1 had to have failed therapy with corticosteroids, immunomodulators or at least one biologic. A total of 51% had failed at least one biologic and 17% had failed both a TNF blocker and an integrin receptor blocker. Of the total population, 46% had failed corticosteroids or immunomodulators but were biologic-naïve and an additional 3% had previously received but had not failed a biologic. At induction baseline and throughout the trial, approximately 52% patients were receiving oral corticosteroids, 28% patients were receiving immunomodulators (AZA, 6-MP, or MTX) and 69% patients were receiving aminosalicylates.
The primary endpoint was clinical remission at Week 8. Clinical remission with a definition of: Mayo stool frequency subscore of 0 or 1, Mayo rectal bleeding subscore of 0 (no rectal bleeding), and Mayo endoscopy subscore of 0 or 1 (Mayo endoscopy subscore of 0 defined as normal or inactive disease and Mayo subscore of 1 defined as presence of erythema, decreased vascular pattern and no friability) is provided in Table 14.
The secondary endpoints were clinical response, endoscopic improvement, and histologic-endoscopic mucosal improvement. Clinical response with a definition of (≥ 2 points and ≥ 30% decrease in modified Mayo score, defined as 3-component Mayo score without the Physician's Global Assessment, with either a decrease from baseline in the rectal bleeding subscore ≥1 or a rectal bleeding subscore of 0 or 1), endoscopic improvement with a definition of Mayo endoscopy subscore of 0 or 1, and histologicÂendoscopic mucosal improvement with a definition of combined endoscopic improvement and histologic improvement of the colon tissue [neutrophil infiltration in <5% of crypts, no crypt destruction, and no erosions, ulcerations, or granulation tissue]) are provided in Table 14.
In UC-1, a significantly greater proportion of patients treated with ustekinumab (at the recommended dose of approximately 6 mg/kg dose) were in clinical remission and response and achieved endoscopic improvement and histologic-endoscopic mucosal improvement compared to placebo (see Table 14).
Table 14: Proportion of Patients Meeting Efficacy Endpoints at Week 8 in UC-1
| Endpoint | Placebo N = 319 |
Ustekinumab† N = 322 |
Treatment difference and 97.5% CIa | ||
| N | % | N | % | ||
| Clinical Remission* | 22 | 7% | 62 | 19% | 12% (7%, 18%)b |
| Bio-naive? | 14/151 | 9% | 36/147 | 24% | |
| Prior biologic failure | 7/161 | 4% | 24/166 | 14% | |
| Endoscopic Improvement§ | 40 | 13% | 80 | 25% | 12% (6%, 19%)b |
| Bio-naive? | 28/151 | 19% | 43/147 | 29% | |
| Prior biologic failure | 11/161 | 7% | 34/166 | 20% | |
| Clinical Response¶ | 99 | 31% | 186 | 58% | 27% (18%, 35%)b |
| Bio-naive? | 55/151 | 36% | 94/147 | 64% | |
| Prior biologic failure | 42/161 | 26% | 86/166 | 52% | |
| Histologic-Endoscopic Mucosal Improvemen‡ | 26 | 8% | 54 | 17% | 9% (3%, 14%)b |
| Bio-naive? | 19/151 | 13% | 30/147 | 20% | |
| Prior biologic failure | 6/161 | 4% | 21/166 | 13% | |
| † Infusion dose of ustekinumab using the weight-based dosage regimen specified in Table 6. ? An additional 7 patients on placebo and 9 patients on ustekinumab (6 mg/kg) had been exposed to, but had not failed, biologics. * Clinical remission was defined as Mayo stool frequency subscore of 0 or 1, Mayo rectal bleeding subscore of 0, and Mayo endoscopy subscore of 0 or 1 (modified so that 1 does not include friability). § Endoscopic improvement was defined as Mayo endoscopy subscore of 0 or 1 (modified so that 1 does not include friability). ¶ Clinical response was defined as a decrease from baseline in the modified Mayo score by ≥30% and ≥2 points, with either a decrease from baseline in the rectal bleeding subscore ≥1or a rectal bleeding subscore of 0 or 1. ‡ Histologic-endoscopic mucosal improvement was defined as combined endoscopic improvement (Mayo endoscopy subscore of 0 or 1) and histologic improvement of the colon tissue (neutrophil infiltration in <5% of crypts, no crypt destruction, and no erosions, ulcerations, or granulation tissue). a Adjusted treatment difference (97.5% CI) b p < 0.001 |
|||||
The relationship of histologic-endoscopic mucosal improvement, as defined in UC-1, at Week 8 to disease progression and long-term outcomes was not evaluated during UC-1.
Rectal Bleeding And Stool Frequency Subscores
Decreases in rectal bleeding and stool frequency subscores were observed as early as Week 2 in ustekinumab-treated patients.
Trial UC-2
The maintenance trial (UC-2) evaluated 523 patients who achieved clinical response 8 weeks following the intravenous administration of either induction dose of ustekinumab in UC-1. These patients were randomized to receive a subcutaneous maintenance regimen of either 90 mg ustekinumab every 8 weeks, or every 12 weeks (a lower dose than recommended), or placebo for 44 weeks.
The primary endpoint was the proportion of patients in clinical remission at Week 44. The secondary endpoints included the proportion of patients maintaining clinical response at Week 44, the proportion of patients with endoscopic improvement at Week 44, the proportion of patients with corticosteroid-free clinical remission at Week 44, and the proportion of patients maintaining clinical remission at Week 44 among patients who achieved clinical remission 8 weeks after induction.
Results of the primary and secondary endpoints at Week 44 in patients treated with ustekinumab at the recommended dosage (90 mg every 8 weeks) compared to the placebo are shown in Table 15.
Table 15: Efficacy Endpoints of Maintenance at Week 44 in UC-2 (52 Weeks from Initiation of the Induction Dose)
| Endpoint | Placebo* N = 175† |
90 mg ustekinumab every 8 weeks N = 176 |
Treatment difference and 95% CI | ||
| N | % | N | % | ||
| Clinical Remission** | 46 | 26% | 79 | 45% | 19% (9%, 28%) a |
| Bio-naive? | 30/84 | 36% | 39/79 | 49% | |
| Prior biologic failure | 16/88 | 18% | 37/91 | 41% | |
| Maintenance of Clinical Response at Week 44† | 84 | 48% | 130 | 74% | 26% (16%, 36%) a |
| Bio-naive? | 49/84 | 58% | 62/79 | 78% | |
| Prior biologic failure | 35/88 | 40% | 64/91 | 70% | |
| Endoscopic Improvement§ | 47 | 27% | 83 | 47% | 20% (11%, 30%) a |
| Bio-naive? | 29/84 | 35% | 42/79 | 53% | |
| Prior biologic failure | 18/88 | 20% | 38/91 | 42% | |
| Corticosteroid-free Clinical Remission‡ | 45 | 26% | 76 | 43% | 17% (8%, 27%) a |
| Bio-naive? | 30/84 | 36% | 38/79 | 48% | |
| Prior biologic failure | 15/88 | 17% | 35/91 | 38% | |
| Maintenance of Clinical Remission at Week 44 in patients who achieved clinical remission 8 weeks after induction | 18/50 | 36% | 27/41 | 66% | 31% (12%, 50%) b |
| Bio-naive? | 12/27 | 44% | 14/20 | 70% | |
| Prior biologic failure | 6/23 | 26% | 12/18 | 67% | |
| ? An additional 3 patients on placebo and 6 patients on ustekinumab had been exposed to, but had not failed, biologics. * The placebo group consisted of patients who were in response to ustekinumab and were randomized to receive placebo at the start of maintenance therapy. ** Clinical remission was defined as Mayo stool frequency subscore of 0 or 1, Mayo rectal bleeding subscore of 0, and Mayo endoscopy subscore of 0 or 1 (modified so that 1 does not include friability). ‡ Clinical response was defined as a decrease from baseline in the modified Mayo score by ≥30% and ≥2 points, with either a decrease from baseline in the rectal bleeding subscore ≥1 or a rectal bleeding subscore of 0 or 1. § Endoscopic improvement was defined as Mayo endoscopy subscore of 0 or 1 (modified so that 1 does not include friability). ‡ Corticosteroid-free clinical remission was defined as patients in clinical remission and not receiving corticosteroids at Week 44. a p =<0.001 b p=0.004 |
|||||
Other Endpoints
Week 16 Responders To Ustekinumab Induction
Patients who were not in clinical response 8 weeks after induction with ustekinumab in UC-1 were not included in the primary efficacy analyses for trial UC-2; however, these patients were eligible to receive a 90 mg subcutaneous injection of ustekinumab at Week 8. Of these patients, 55/101 (54%) achieved clinical response eight weeks later (Week 16) and received ustekinumab 90 mg subcutaneously every 8 weeks during the UC-2 trial. At Week 44, there were 97/157 (62%) patients who maintained clinical response and there were 51/157 (32%) who achieved clinical remission.
Histologic-Endoscopic Mucosal Improvement At Week 44
The proportion of patients achieving histologic-endoscopic mucosal improvement during maintenance treatment in UC-2 was 75/172 (44%) among patients on ustekinumab and 40/172 (23%) in patients on placebo at Week 44. The relationship of histologic-endoscopic mucosal improvement, as defined in UCÂ2, at Week 44 to progression of disease or long-term outcomes was not evaluated in UC-2.
Endoscopic Normalization
Normalization of endoscopic appearance of the mucosa was defined as a Mayo endoscopic subscore of 0. At Week 8 in UC-1, endoscopic normalization was achieved in 25/322 (8%) of patients treated with ustekinumab and 12/319 (4%) of patients in the placebo group. At Week 44 of UC-2, endoscopic normalization was achieved in 51/176 (29%) of patients treated with ustekinumab and in 32/175 (18%) of patients in placebo group.
Patient Information for Pyzchiva
PYZCHIVA®
(Piz-chi-va)
(ustekinumab-ttwe) injection, for subcutaneous or intravenous use
What is the most important information I should know about PYZCHIVA?
PYZCHIVA is a medicine that affects your immune system. PYZCHIVA can increase your risk of having serious side effects, including:
Serious infections: PYZCHIVA may lower the ability of your immune system to fight infections and may increase your risk of infections. Some people have serious infections while taking ustekinumab products, including tuberculosis (TB), and infections caused by bacteria, fungi, or viruses. Some people have to be hospitalized for treatment of their infection.
- Your doctor should check you for TB before starting PYZCHIVA.
- If your doctor feels that you are at risk for TB, you may be treated with medicine for TB before you begin treatment with PYZCHIVA and during treatment with PYZCHIVA.
- Your doctor should watch you closely for signs and symptoms of TB while you are being treated with PYZCHIVA.
You should not start taking PYZCHIVA if you have any kind of infection unless your doctor says it is okay.
Before starting PYZCHIVA, tell your doctor if you:
- think you have an infection or have symptoms of an infection such as:
- fever, sweat, or chills
- weight loss
- muscle aches
- warm, red, or painful skin or sores on your body
- cough
- diarrhea or stomach pain
- shortness of breath
- burning when you urinate or urinate more often than normal
- blood in phlegm
- feel very tired
- are being treated for an infection or have any open cuts.
- get a lot of infections or have infections that keep coming back.
- have TB, or have been in close contact with someone with TB.
After starting PYZCHIVA, call your doctor right away if you have any symptoms of an infection (see above). These may be signs of infections such as chest infections, or skin infections or shingles that could have serious complications. PYZCHIVA can make you more likely to get infections or make an infection that you have worse. People who have a genetic problem where the body does not make any of the proteins interleukin 12 (IL-12) and interleukin 23 (IL-23) are at a higher risk for certain serious infections. These infections can spread throughout the body and cause death. People who take PYZCHIVA may also be more likely to get these infections.
Cancers. PYZCHIVA may decrease the activity of your immune system and increase your risk for certain types of cancers. Tell your doctor if you have ever had any type of cancer. Some people who are receiving ustekinumab products and have risk factors for skin cancer have developed certain types of skin cancers. During your treatment with PYZCHIVA, tell your doctor if you develop any new skin growths.
Posterior Reversible Encephalopathy Syndrome (PRES). PRES is a rare condition that affects the brain and can cause death. The cause of PRES is not known. If PRES is found early and treated, most people recover. Tell your doctor right away if you have any new or worsening medical problems including:
- headache
- confusion
- seizures
- vision problems
What is PYZCHIVA?
PYZCHIVA is a prescription medicine used to treat:
- adults and children 6 years and older with moderate or severe psoriasis who may benefit from taking injections or pills (systemic therapy) or phototherapy (treatment using ultraviolet light alone or with pills).
- adults and children 6 years and older with active psoriatic arthritis.
- adults 18 years and older with moderately to severely active Crohn's disease.
- adults 18 years and older with moderately to severely active ulcerative colitis.
It is not known if PYZCHIVA is safe and effective in children less than 6 years of age.
Do not take PYZCHIVA if you are allergic to ustekinumab products or any of the ingredients in PYZCHIVA. See the end of this Medication Guide for a complete list of ingredients in PYZCHIVA.
Before you receive PYZCHIVA, tell your doctor about all of your medical conditions, including if you:
- have any of the conditions or symptoms listed in the section “What is the most important information I should know about PYZCHIVA?”
- ever had an allergic reaction to ustekinumab products. Ask your doctor if you are not sure.
- have recently received or are scheduled to receive an immunization (vaccine). People who take PYZCHIVA should not receive live vaccines. Tell your doctor if anyone in your house needs a live vaccine. The viruses used in some types of live vaccines can spread to people with a weakened immune system, and can cause serious problems. You should not receive the BCG vaccine during the one year before receiving PYZCHIVA or one year after you stop receiving PYZCHIVA.
- have any new or changing lesions within psoriasis areas or on normal skin.
- are receiving or have received allergy shots, especially for serious allergic reactions. Allergy shots may not work as well for you during treatment with PYZCHIVA. PYZCHIVA may also increase your risk of having an allergic reaction to an allergy shot.
- receive or have received phototherapy for your psoriasis.
- are pregnant or plan to become pregnant. It is not known if PYZCHIVA can harm your unborn baby. You and your doctor should decide if you will receive PYZCHIVA. See “What should I avoid while using PYZCHIVA?”
- received PYZCHIVA while you were pregnant. It is important that you tell your baby’s healthcare provider before any vaccinations are given to your baby.
- are breastfeeding or plan to breastfeed. PYZCHIVA can pass into your breast milk.
Talk to your doctor about the best way to feed your baby if you receive PYZCHIVA.
Tell your doctor about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements.
Know the medicines you take. Keep a list of them to show your doctor and pharmacist when you get a new medicine.
How should I use PYZCHIVA?
- Use PYZCHIVA exactly as your doctor tells you to.
- Adults with Crohn's disease and ulcerative colitis will receive the first dose of PYZCHIVA through a vein in the arm (intravenous infusion) in a healthcare facility by a healthcare provider. It takes at least 1 hour to receive the full dose of medicine. You will then receive PYZCHIVA as an injection under the skin (subcutaneous injection) 8 weeks after the first dose of PYZCHIVA, as described below.
- Adults with psoriasis or psoriatic arthritis and children 6 years and older with psoriasis or psoriatic arthritis will receive PYZCHIVA as an injection under the skin (subcutaneous injection) as described below.
- Injecting PYZCHIVA under your skin
- PYZCHIVA is intended for use under the guidance and supervision of your doctor. In children 6 years and older, it is recommended that PYZCHIVA be administered by a healthcare provider. If your doctor decides that you or a caregiver may give your injections of PYZCHIVA at home, you should receive training on the right way to prepare and inject PYZCHIVA. Your doctor will determine the right dose of PYZCHIVA for you, the amount for each injection, and how often you should receive it. Do not try to inject PYZCHIVA yourself until you or your caregiver have been shown how to inject PYZCHIVA by your doctor or nurse.
- Inject PYZCHIVA under the skin (subcutaneous injection) in your upper arms, buttocks, upper legs (thighs) or stomach area (abdomen).
- Do not give an injection in an area of the skin that is tender, bruised, red or hard.
- Use a different injection site each time you use PYZCHIVA.
- If you inject more PYZCHIVA than prescribed, call your doctor right away.
- Be sure to keep all of your scheduled follow-up appointments.
Read the detailed Instructions for Use at the end of this Medication Guide for instructions about how to prepare and inject a dose of PYZCHIVA, and how to properly throw away (dispose of) used needles and syringes. The syringe, needle and vial must never be re-used. After the rubber stopper is punctured, PYZCHIVA can become contaminated by harmful bacteria which could cause an infection if re-used. Therefore, throw away any unused portion of PYZCHIVA.
What should I avoid while using PYZCHIVA?
You should not receive a live vaccine while taking PYZCHIVA. See “Before you receive PYZCHIVA, tell your doctor about all of your medical conditions, including if you:”
What are the possible side effects of PYZCHIVA?
PYZCHIVA may cause serious side effects, including:
- See “What is the most important information I should know about PYZCHIVA?”
- Serious allergic reactions. Serious allergic reactions can occur with PYZCHIVA. Stop using PYZCHIVA and get medical help right away if you have any of the following symptoms of a serious allergic reaction:
- feeling faint
- chest tightness
- swelling of your face, eyelids, tongue, or throat
- skin rash
- Lung inflammation. Cases of lung inflammation have happened in some people who receive ustekinumab products, and may be serious. These lung problems may need to be treated in a hospital. Tell your doctor right away if you develop shortness of breath or a cough that doesn't go away during treatment with PYZCHIVA.
Common side effects of PYZCHIVA include:
- nasal congestion, sore throat, and runny nose
- redness at the injection site
- upper respiratory infections
- vaginal yeast infections
- fever
- urinary tract infections
- headache
- sinus infection
- tiredness
- bronchitis
- itching
- diarrhea
- nausea and vomiting
- stomach pain
These are not all of the possible side effects of PYZCHIVA. Call your doctor for medical advice about side effects.
You may report side effects to FDA at 1-800-FDA-1088. You may also report side effects to Sandoz Inc. at 1-800-525-8747.
How should I store PYZCHIVA?
- Store PYZCHIVA vials and prefilled syringes in a refrigerator between 36°F to 46°F (2°C to 8°C).
- Store PYZCHIVA vials standing up straight.
- Store PYZCHIVA in the original carton to protect it from light until time to use it.
- Do not freeze PYZCHIVA.
- Do not shake PYZCHIVA.
- If needed, individual PYZCHIVA prefilled syringes may be stored at room temperature up to 86°F (30°C) for a maximum single period of up to 60 days in the original carton to protect from light.
- Record the date when the prefilled syringe is first removed from the refrigerator on the carton in the space provided.
- You may return the prefilled syringe to the refrigerator 1 time only for a maximum of 3 days, either during the 60day period or at the end of the 60-day period.
- Record the date when the prefilled syringe is returned to the refrigerator on the carton.
- Discard the prefilled syringe if not used within 60 days of room temperature storage and you did not return it to the refrigerator, or if it has been returned to the refrigerator and is not used within 3 days.
- Do not use PYZCHIVA after the expiration date on the carton or on the prefilled syringe.
Keep PYZCHIVA and all medicines out of the reach of children.
General information about the safe and effective use of PYZCHIVA.
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use PYZCHIVA for a condition for which it was not prescribed. Do not give PYZCHIVA to other people, even if they have the same symptoms that you have. It may harm them. You can ask your doctor or pharmacist for information about PYZCHIVA that was written for health professionals.
What are the ingredients in PYZCHIVA?
Active ingredient: ustekinumab-ttwe
Inactive ingredients: Single-dose prefilled syringe for subcutaneous use contains histidine, histidine hydrochloride monohydrate, polysorbate 80, and sucrose. Single-dose vial for intravenous infusion contains edetate disodium, histidine, histidine hydrochloride monohydrate, methionine, polysorbate 80, and sucrose.
INSTRUCTIONS FOR USE
PYZCHIVA®
(Piz-chi-va)
(ustekinumab-ttwe) injection, for subcutaneous use
Instructions for injecting PYZCHIVA using a prefilled syringe.
Read this Instructions for Use before you start using PYZCHIVA. Your doctor or nurse should show you how to prepare and give your injection of PYZCHIVA the right way.
If you cannot give yourself the injection:
- ask your doctor or nurse to help you, or
- ask someone who has been trained by a doctor or nurse to give your injections.
Do not try to inject PYZCHIVA yourself until you have been shown how to inject PYZCHIVA by your doctor, nurse or health professional.
Important information:
- Before you start, check the carton to make sure that it is the right dose. You will have either 45 mg or 90 mg as prescribed by your doctor.
- If your dose is 45 mg, you will receive one 45 mg prefilled syringe.
- If your dose is 90 mg, you will receive either one 90 mg prefilled syringe or two 45 mg prefilled syringes. If you receive two 45 mg prefilled syringes for a 90 mg dose, you will need to give yourself two injections, one right after the other.
- Children 12 years of age and older with psoriasis who weigh 132 pounds (60 kg) or more may use a prefilled syringe.
- Store PYZCHIVA in a refrigerator between 36°F to 46°F (2°C to 8°C).
- If needed, individual prefilled syringes may be stored at room temperature up to 86°F (30°C) for a maximum single period of up to 60 days in the original carton to protect from light.
- Record the date when the prefilled syringe is removed from the refrigerator on the carton in the space provided.
- You may return the prefilled syringe to the refrigerator 1 time only for a maximum of 3 days, either during the 60-day period or at the end of the 60-day period.
- Record the date when the prefilled syringe is returned to the refrigerator on the carton.
- Discard the prefilled syringe if not used within 60 days of room temperature storage and you did not return it to the refrigerator, or if it has been returned to the refrigerator and is not used within 3 days.
- Check the expiration date on the prefilled syringe and carton. Do not use PYZCHIVA after the expiration date has passed. If the expiration date has passed or if the prefilled syringe has been stored above 86°F (30°C), call your doctor or pharmacist, or call 1-800-5258747 for help.
- Make sure the syringe is not damaged. Do not use the prefilled syringe if it is damaged.
- Check your prefilled syringe for any particles or discoloration. Your prefilled syringe should look clear and colorless to light yellow.
- Do not use if it is frozen, discolored, cloudy or has particles. Get a new prefilled syringe.
- Do not shake the prefilled syringe at any time. Shaking your prefilled syringe may damage your PYZCHIVA medicine. If your prefilled syringe has been shaken, do not use it. Get a new prefilled syringe.
- To reduce the risk of accidental needle sticks, each prefilled syringe has a needle guard that is automatically activated to cover the needle after you have given your injection. Do not pull back on the plunger at any time.
Gather the supplies you will need to prepare and to give your injection. (See Figure A) Â You will need:
- antiseptic wipes
- cotton balls or gauze pads adhesive bandage
- your prescribed dose of PYZCHIVA (See Figure B)
- FDA-cleared sharps disposal container. See “Step 4: Dispose of the syringe.”
Figure A
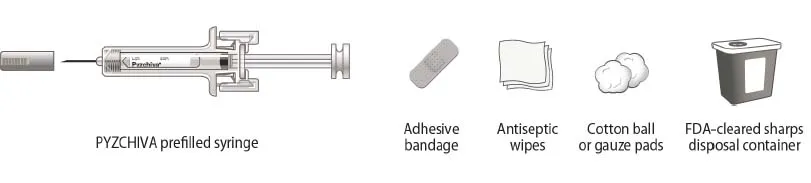 |
Figure B
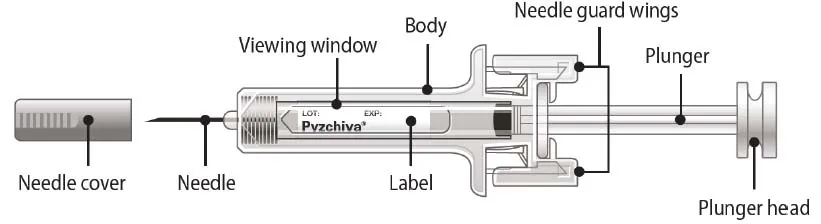 |
Step 1: Prepare the injection
- Choose a well-lit, clean, flat work surface.
- For a more comfortable injection, leave PYZCHIVA prefilled syringe at room temperature for about 30 minutes before injecting. Do not warm the prefilled syringe in any other way (for example, do not warm it in a microwave or in hot water).
- Wash your hands well with soap and warm water.
- Hold the prefilled syringe with the covered needle pointing upward.
Step 2: Prepare your injection site
- Choose an injection site around your stomach area (abdomen), buttocks, upper legs (thighs). If a caregiver is giving you the injection, the outer area of the upper arms may also be used. (See Figure C)
- Use a different injection site for each injection. Do not give an injection in an area of the skin that is tender, bruised, red or hard.
- Clean the skin with an antiseptic wipe where you plan to give your injection.
- Do not touch this area again before giving the injection. Let your skin dry before injecting.
- Do not fan or blow on the clean area.
Figure C
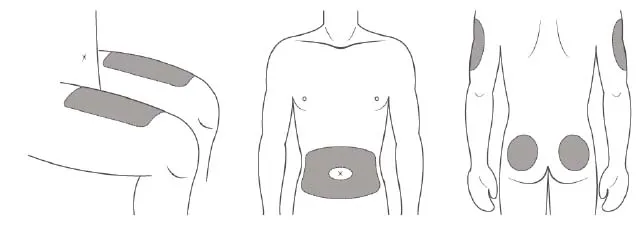 |
*Areas in gray are recommended injection sites.
Step 3: Inject PYZCHIVA
- Remove the needle cover when you are ready to inject your PYZCHIVA.
- Do not touch the plunger or plunger head while removing the needle cover.
- Hold the body of the prefilled syringe with one hand, and pull the needle cover straight off. Â (See Figure D)
- Put the needle cover in the trash.
- You may also see a drop of liquid at the end of the needle. This is normal.
- Do not touch the needle or let it touch anything.
- Do not use the prefilled syringe if it is dropped without the needle cover in place. Call your doctor, nurse or health professional for instructions.
Figure D
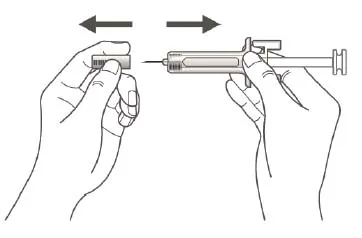 |
- Hold the body of the prefilled syringe in one hand between the thumb and index fingers. (See Figure E)
Figure E
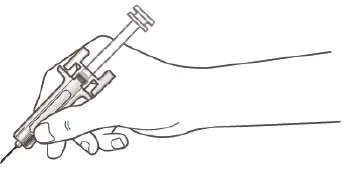 |
- Do not pull back on the plunger at any time.
- Use the other hand to gently pinch the cleaned area of skin. Hold firmly.
- Use a quick, dart-like motion to insert the needle into the pinched skin at about a 45-degree angle. (See Figure F)
Figure F
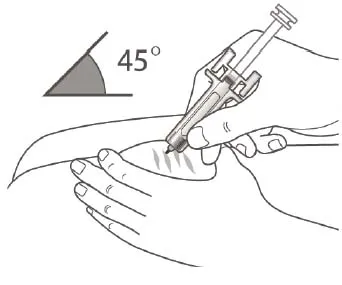 |
- Inject all of the liquid by using your thumb to push in the plunger until the plunger head is completely between the needle guard wings. (See Figure G)
Figure G
 |
- When the plunger is pushed as far as it will go, keep pressure on the plunger head. Take the needle out of the skin and let go of the skin.
- Slowly take your thumb off the plunger head. This will let the empty syringe move up until the entire needle is covered by the needle guard. (See Figure H)
Figure H
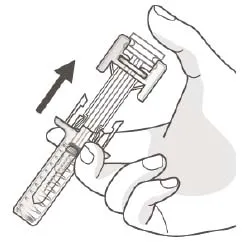 |
- When the needle is pulled out of your skin, there may be a little bleeding at the injection site. This is normal. You can press a cotton ball or gauze pad to the injection site if needed. Do not rub the injection site. You may cover the injection site with a small adhesive bandage, if necessary.
If your dose is 90 mg, you will receive either one 90 mg prefilled syringe or two 45 mg prefilled syringes. If you receive two 45 mg prefilled syringes for a 90 mg dose, you will need to give yourself a second injection right after the first. Repeat Steps 1–3 for the second injection using a new syringe. Choose a different site for the second injection.
Step 4: Dispose of the syringe.
- Put the syringe in a FDA-cleared sharps disposal container right away after use. Do not throw away (dispose of) loose syringes in your household trash.
- If you do not have a FDA-cleared sharps disposal container, you may use a household container that is:
- made of heavy-duty plastic.
- can be closed with a tight-fitting, puncture-resistant lid, without sharps being able to come out.
- upright and stable during use,
- leak-resistant,
- and properly labeled to warn of hazardous waste inside the container.
- When your sharps disposal container is almost full, you will need to follow your community guidelines for the right way to dispose of your sharps disposal container. There may be local or state laws about how to throw away syringes and needles. For more information about safe sharps disposal, and for specific information about sharps disposal in the state that you live in, go to the FDA's website at: http://www.fda.gov/safesharpsdisposal.
- Do not dispose of your sharps disposal container in your household trash unless your community guidelines permit this. Do not recycle your sharps disposal container.
- If you have any questions, talk to your doctor or pharmacist.
Keep PYZCHIVA and all medicines out of the reach of children.
This Instructions for Use has been approved by the U.S. Food and Drug Administration.
From 
Report Problems to the Food and Drug Administration
You are encouraged to report negative side effects of prescription drugs to the FDA. Visit the FDA MedWatch website or call 1-800-FDA-1088.